About the Achilles Tendon
The Achilles Tendon is the strongest and largest tendon in the body. It is extremely vulnerable to injury due to its limited blood supply and the numerous forces to which it is subjected.
The Achilles Tendon is known as a co-joined tendon. This tendon joins directly into the calf muscles (gastrocnemius and soleus). The Achilles Tendon transmits the force generated by the calf muscles to produce the push-off required for walking, running, and jumping.
The area of the Achilles Tendon (approximately 2 to 6 cm above its insertion into the calcaneus) is very dense and under constant tension; consequently, this area has the poorest blood supply, which makes it extremely susceptible to injury and very slow to heal when it is injured.
The calf muscles associated with the Achilles Tendon are composed of several layers of muscles, with the large gastrocnemius and soleus muscles being the more superficial. Under these muscles is a deeper layer of three muscles – the tibialis posterior, flexor hallucis longus, and flexor digitorum longus. Injuries, restrictions, or adhesions in any of these tissue structures can directly affect the function and strength of the Achilles Tendon.
Kinetic Chain Structures of the Achilles Tendon
Other structures of the Achilles Tendon’s kinetic chain that are commonly involved in Achilles Tendon injuries include:
- The hamstrings, which are a group of muscles that include the biceps femoris, semitendinosus, and semimembranosus. Tension in these muscles causes increased stress upon the muscles of the lower leg.
- The tibialis posterior, which lies deep within/to the calf muscles. This muscle inverts the foot (turns the foot inwards) and plantar flexes the foot (helps you to point your toes down).
- The popliteus muscle, which lies deep behind the knee and is involved in medial knee rotation. When it is restricted, it may place increased stress upon the lower extremities.
- The soleus muscle, which is a powerful plantar flexor of the foot and gives you the ability to rise up on your toes.
- The flexor digitorum longus which works to flex toes 2 thru 5. It also helps to plantar flex the foot.
- The flexor hallucis longus, flexor hallucis brevis, and the tibialis anterior muscles, which are all involved in cases of increased pronation and hyperpronation.
- The plantaris muscle, which inserts into the middle one third of the posterior calcaneal surface (heel bone), just on the inside of the Achilles Tendon. This muscle assists in plantar flexion of the foot and is also involved in flexion of the leg.
{kind=link}
{kind=link}
{kind=link}
What is Achilles Tendonitis or Tendinopathy
The term Achilles Tendonitis (“itis” implying the presence of inflammation) is commonly used to describe tenderness, pain, and swelling in the area just above the heel bone (2 to 6 cm above the calcaneus). A more accurate term would be Achilles Tendinopathy which identifies the presence of both tendonitis (inflammation) and tendinosis (small tears in surrounding tissue).
In our clinic, we typically see three types of injuries to the Achilles Tendon – paratenonitis, tendinosis, and rupture of the tendons:
Achilles Tendonitis/Paratenonitis: This injury is commonly known as Achilles Tendonitis and describes an inflammation of the paratenon - a sheath surrounding the Achilles Tendon. Paratenonitis is often caused by overuse or repetitive strain and commonly occurs in triathletes and runners.
Tendinosis: Refers to degeneration within the Achilles Tendon due to a previous tear. This condition can be felt as a palpable tendon nodule very close to the heel. The nodule is formed by the accumulation of scar tissue.
Circulation to the Achilles Tendon is very poor, especially near the heel, resulting in poor oxygen supply. This results in poor healing and formation of microscopic tears, causing the tendon to thicken. Chronic Achilles Tendinosis can lead to a complete rupture of the tendon if it is not treated and rehabilitated correctly. If not addressed, this tendinosis may be a warning sign of worse things to come.
Rupture of the Tendon (either partial or complete): Refers to the tearing or separation of the Achilles Tendon from the calcaneus (heel bone). The Achilles Tendon is very strong and can withstand a force of 1000 pounds without tearing. However, even with this strength, the Achilles Tendon is the second most frequently ruptured tendon in the body. A complete rupture is where the tendon has completely separated from the calcaneus (heel bone). This can occur when either Paratenonitis and Tendinosis are not correctly treated and rehabilitated. Surgical intervention is the only solution for resolving a complete rupture of the Achilles Tendon.
Biomechanical Analysis in Resolving Achilles Tendonitis
Biomechanical analysis is an essential tool when trying to determine exactly which areas of the patient’s kinetic chain need to be addressed during treatment. Through careful observation of the abnormal motions in a person’s gait, we can identify the key areas that require treatment, and use this to determine which combination of exercises can most effectively help to resolve this condition. What appears to be a simple case of Achilles Tendonitis could involve structures from the foot right up into your core.
Let’s take a look at the following two motion-change examples, and learn how deviations in each one can cause injuries to the Achilles Tendon:
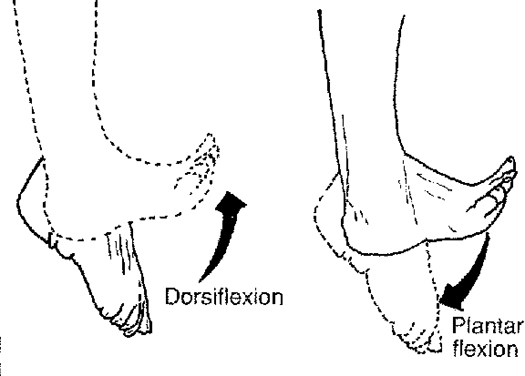
Effects of Abnormal Plantar Flexion
Plantar flexion describes the downward movement of the foot (calf raise). The strongest muscle group in your leg - the triceps surae - performs much of the plantar flexion. The triceps surae is composed of the by the soleus (deepest calf muscles) and the gastrocnemius (superficial double headed calf muscle). Both these muscles form the Achilles tendon, which then attaches to the posterior surface of your heel bone (calcaneus). When these muscles contract (or shorten) they pull your heel bone up, and push your toe down.
Pain, restrictions, tightness in these structures, or abnormal motion during plantar flexion is often the immediate cause of Achilles Tendonitis. In some cases, these same structures may also be affected by knee function and stability since the gastrocnemius muscle crosses three joints – knee, ankle, and subtalar joints. Alterations in the function of any of these joints will also have the immediate effect of increasing tension on the Achilles tendon.
Effects of Abnormal or Restricted Knee Flexion
Another common cause of Achilles Tendonitis are restrictions and injuries to the hamstrings. The hamstrings are the antagonists to the knee flexors. Restrictions in your hamstrings often prevents the full extension of your knee, resulting in increased tension in the Achilles tendon. Hamstring restrictions can create restrictions and tightness in the calf muscles, which in turn tightens the Achilles tendon.
Resolving Achilles Tendonitis
It is easy to see how a restriction in one area can cascade and develop into multiple restrictions within other associated structures. The key to resolving Achilles Tendonitis is to remove all these restrictions – along the entire kinetic chain – not just at the point of pain. Soft tissue therapy (ART, Graston, Registered Massage Therapy, Fascial Manipulation) can be very effective at doing this, but it requires someone who is trained in biomechanical analysis to locate all the affected areas.
Key Point: The location of these restrictions, or weak links, will vary from person to person. Each individual may present with the same diagnosis of Achilles Tendonitis, but the areas of restriction will often be completely different, and thus require completely different treatments.
In addition to removing and releasing these restrictions, it is important to use exercise to rehabilitate, strengthen, and restore the function of all the structures in this kinetic chain.
If you would like more information or to purchase our books please go to www.releaseyourbody.com .
If you would like information about our clinic in Calgary Alberta please go to www.kinetichealth.ca.
(COPYRIGHT KINETIC HEALTH 2012 – ALL RIGHTS RESERVED)
No comments:
Post a Comment